Talus is second largest tarsal bone of foot forms ankle joint. Dome of the talus forms ankle joint. The cartilage covering of dome is one of the thickest articular cartilage of the body. The thickness is one eight of an Inch. OCD or osteochondral lesion of talus is a condition that affects cartilage and its underlying bone at inner and outer corner of talar dome. OCD can happen at any age and usually associated with a history of ankle sprain or fracture. OCD can also happen due to chronic repetitive microtrauma can create ischemic environment of a patch of cartilage and its underlying bone and develops OCD. A patch of cartilage flap gets detached from underlying bone following ankle injury which become avascular and develops OCD.
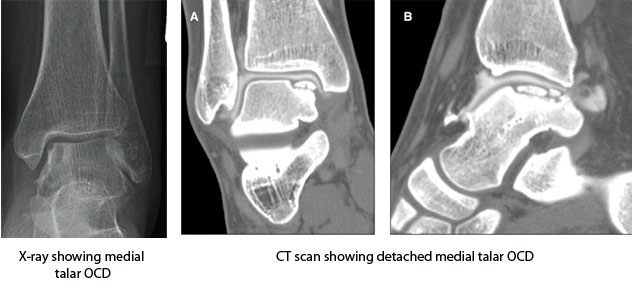
Clinical symptom represents dull pain, swelling and stiffness of ankle. May have mechanical symptom like catching or locking. Initially it mimics an ankle sprain. There is no specific clinical finding related to talus OCD. It can remain asymptomatic for long and detect incidentally when x-ray is done for some other reason. This asymptomatic lesion can become symptomatic following an ankle injury. X-ray can diagnose an established OCD whereas MRI is helpful in early one where findings are not significant enough to identifiable in x-ray. Medial OCD is deep and large whereas lateral one is small and superficial. Medial lesions are more common than lateral. Chronic ankle instability and cavo-varus feet are prone to develop OCD.

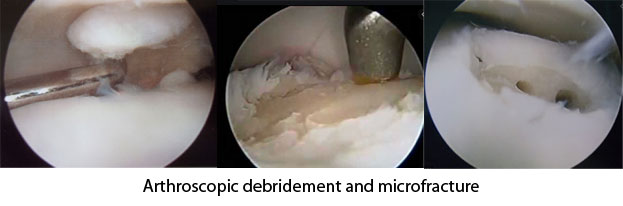
Treatment of OCD depends on age of onset, duration of symptom and severity of involvement (staging) detected on imaging. In early stage of disease treatment is immobilization of ankle in plaster cast or pneumatic boot and non-weight bearing for 6-8 weeks followed by physical therapy. Surgical treatment is recommended in advanced disease where the cartilage flap become totally detached or in cases where symptoms are not subsiding with conservative treatment. Surgical treatment options are: