


Knee cap plays a major role in knee movements well as our daily activity. It is the point through which body weight and forces transfer to help in activities like squatting, climbing up & down etc. During this activity knee cap moves along the center of the knee joint. If knee cap off tracks during knee movement cause instability of knee cap. It is a major concern specially in young population. Overall incidence is 1 per 1,000,000 with higher incidence at second decade, which is 30 per 1,000,000 and significantly low after the age of 30. Knee cap instability mostly occurs among young athletic male while performing sports activity as well as in overweight adolescent female.
Knee cap instability ranges from mild tilting to subluxation or complete dislocation at lateral side. Various factors are responsible for keeping it in track within center of the knee joint while knee movement. These factors are different static and dynamic soft tissue stabilizer around the knee cap, shape of knee cap and thigh bone in relation to knee cap and overall alignment of the lower limb. Deviation of these factors from normal put the knee cap at risk of instability.
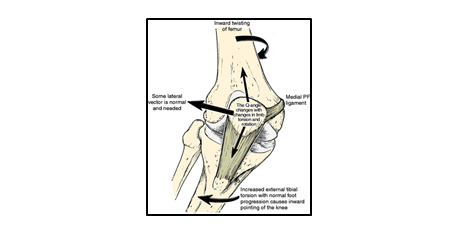
Different tissue forces that balances patellar stability and tracking patellofemoral movement
Followings are the different conditions which can cause Knee cap instability as a sole factor or in combination
Knee cap instability presents either as acute injury or chronic recurrent dislocation or instability. Acute dislocation is a traumatic event mostly occurs during sports or recreation activity. There is a feeling of POP or SNAP followed by acute pain and swelling of knee joint. Most of the time knee comes back to its position when leg gets straight. Some times knee cap may get stuck at outer aspect of knee. Physical examination may not be possible due to apprehension from acute pain and swelling due to bleeding inside knee joint. There may be bruise or ecchymosis on medial aspect of knee joint. Knee cap may get displaced on outer aspect on manipulation. These injuries need to be evaluated for fractures or other ligamentous injury of knee joint. And required immediate active attention to relieve the pain. In acute dislocation medial patellofemoral ligament invariably get injured; mostly complete tear sometimes partial tear. The other injury is osteochondral fracture of patella.
Recurrent dislocation is more indolent form and usually never present with acute symptom. Most of the time they give a history of giving way of knee joint which get corrected automatically. There may be a previous history of acute dislocation. But in others the presentation is very vague. There may be sensation of giving way, weakness, difficulty in negotiating staircase and inability to perform sports or recreation activity. Physical examination is done to look for limb alignment, rotational malalignment, tracking of knee cap while knee movement, mediolateral instability of knee cap.
Based on the finding on clinical examination different imaging is required like plain X-ray of knee joint, limb alignment x-ray, MRI of knee joint, CT scan. Different measurements are being evaluated in these imaging to identify the presence and extend of the deformity.
In acute dislocation if there is no osteochondral fracture, underlying bony deformity or limb alignment issue the treatment is conservative for 1st time dislocation. These are Immobilization, icepack, analgesic, aspiration of hemarthrosis. After subsidence of acute swelling and pain physiotherapy rehabilitation is started to restore the mobility and joint function. Most common surgery performed in acute dislocation is fixation of osteochondral fragment and MPFL reconstruction.
In recurrent dislocation different surgical modalities may require to restore the abnormal anatomy predisposing the condition.
These surgical procedures may require individually or in combination depending on the presence of abnormality detected in different radiological evaluation.



