


This essentially stands for loss of blood supply to the ball of hip joint. The reason for the ball of hip joint getting affected is mainly to do with the pattern of supply. The normal sequence of events following the blood supply cut off is due to the changes in the structure and the make up off the bone. The weakening of the structure of the bone takes place over few months and sometimes even years. It loses its inherent architecture and can collapse under the weight of the body or the force on the bone itself. As most of these areas are within the joint, they can actually cause disruption of the smooth articular surfaces of the bone leading to prolonged problems and complications. The bone however can revascularize, itself which is to say that the blood supply can start again but the period in which it will start is not very certain but there is no doubt about the capacity of the bone to regenerate. If the bone however collapses in the meanwhile, then arthritis would be inevitable.
The age of onset of symptoms can be very variable depending on the moon involved and the cause for the am we in. hey yes much more common in the younger age group the consequence this is can also be significant in that age group.
Symptoms of AVN
In its early stages, AVN may not cause symptoms. As blood cells die and the disease progresses, symptoms may occur in roughly this order:
Pain may dramatically increase in intensity because of tiny breaks in the bone, called microfractures. These can cause the bone to collapse. Ultimately, the joint may break down and develop arthritis.
The time between the first symptoms and the inability to move a joint varies. In general, it ranges from a few months to more than a year. Symptoms may appear bilaterally, meaning on both sides of the body.

Late sequelae of AVN of hip. Collapsed head of femur with arthritis.
Causes and risk factors for the condition
Injury around hip like fracture neck of femur and hip dislocation slows or stops blood flow to the ball of hip joint is the main cause of AVN. Other common risks and causes of AVN are:
Some fewer common causes of AVN include:
Some times no symptoms could be found to be the cause of AVN. This condition is called idiopathic AVN.
Men develop AVN more than women unless the cause is injury or lupus. It most often affects people aged between 30-60 yrs. of age. But people of any age can develop AVN.
Stages of AVN:

Avascular necrosis (AVN)
Prognosis for Avascular Necrosis
More than half the people with this condition need surgery within 3 years of diagnosis. If a bone collapse in one of the joints, it is very likely to it happen in another as well.
Patients outcome depends on several factors, like
Patients are less likely to do well if:
Treatment
The treatment of this condition really depends on the age of the patient, the amount of disability that the patient has and the stage that the patient is in. Ideally every doctor would like to see the full regeneration of the bone and the full restoration of the normal anatomy. Unfortunately, most people will come at stage when the bone surfaces are already destroyed.
In the early stage's procedures like Core decompression and Bone grafting, Stem cell therapy and PRP therapy have all been tried with varying degrees of success. In the earlier stages these are the most recommended procedures and can save the patient a lot of trouble in later life. All these procedures are fairly less invasive and do not involve any prolonged treatment. Most patients are also given medications such as Bisphosphonates (e.g. Zoledronate and Alendronate therapy) which could preserve some of the bone structure.
Bone Marrow Aspirate Concentrate (BMAC) and injection of progenitor stem cells has been now carried out extensively and with some degree of refinement may be the best option in this situation.
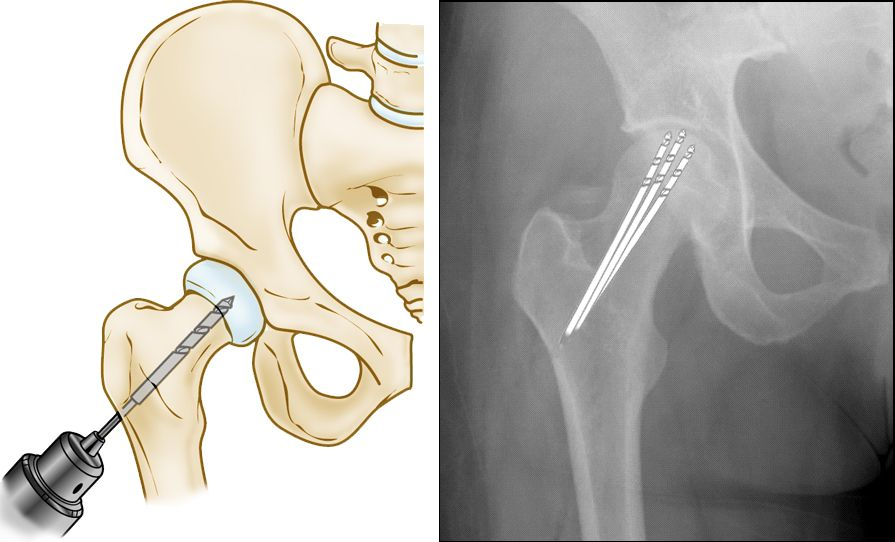
It does involve making very small cut on the side of the hip inserting guidewire to reach the spot where the AVN is localized, drilling it multiple times, cleaning out the dead bone and replacing it with live cells which would hopefully regenerate the hip bone.
Role of BMAC (Bone Marrow Aspirate Concentrate)
Bone Marrow Aspirate Stem Cell Concentrate (BMAC) is a component of your bone marrow that contains growth factors and anti-inflammatory proteins which have been shown to promote bone and soft tissue healing as well as reduce symptoms of pain related to injuries, tendinitis and arthritis.
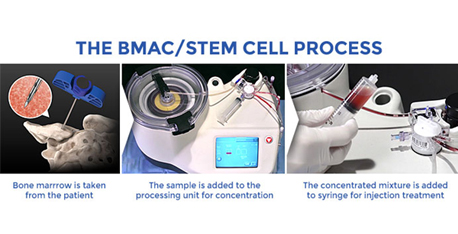
Stem cells can be found in many tissues throughout your body, but one of the richest sources can be found in your bone marrow. Fortunately, bone marrow can be harvested from several bones within your body and is relatively easy to access. Bone marrow is aspirated through a small needle puncture in Pelvic bone and placed in a special processing unit, which concentrate your body’s stem cells, platelets and growth factors. The concentrate is collected into a sterile syringe and injected into the targeted body area being treated.
BMAC may be recommended typically for patients that have failed other conservative therapies including physical therapy, medications, rest, and other injections. It is also a good option for those that are not candidates for surgery or prefer to avoid elective surgery.
Most patients begin to see improvement approximately 4 to 8 weeks after treatment, with an increase in strength and stability, along with a reduced amount of pain. However, recovery time can vary significantly depending on the extent of deterioration from chronic or acute condition. An estimate can be made but by no means is it an accurate timeline. Some prognosis can be also offered depending on the diagnosis.
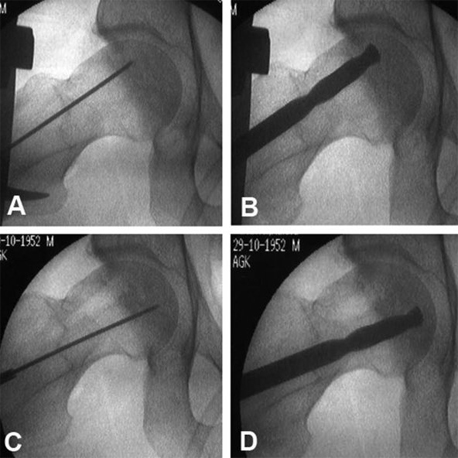
Figure: Intra operative photographs showing the site being reached and localised and a wire inserted through the bone to reach it. The drill is then threaded on top of this wire and the affected areas are then drilled to remove the unhealthy bone . This is also called core decompression. After this the dead and drilled areas can be filled with bone marrow or BMAC or PRP.
Bone marrow injections into the area have also been tried along with PRP and Adipose cell derived cells and are still within experimental options for this condition.
Once the patient reaches a later stage of the disease and the head is already collapsed then the only option left would be to do a joint replacement. Hip Joint Replacement is highly successful operation.
Total hip replacement in AVN
In the majority of the patients the hip replacement itself is not a very difficult operation especially for this condition as the anatomy before the condition started was fairly normal and the patients normally will come in before too much destruction having happened. The challenge in these cases is young age of majority of these patients. So, the operation done should last them throughout their life or as long as possible with almost normal function and preserving as much bone as able.
The surgical technique and the choice of implant hence becomes fairly important for the long term survival and function of the patient. The preference in majority of these patients is hence uncemented total hip replacement with articular surfaces such as ceramic against a Plastic Cup or a Ceramic Cup. Both of these options have been giving us wonderful results and are fairly commonly used. The implants from some of the American Orthopaedic companies such as Zimmer- Biomet, Smith & Nephew, Stryker and DuPuy are well established and give excellent results in the long term. We have patients operated even 14 to 15 years back who have not reported any issues with their replacements using these articular surfaces. The operation in these patients requires almost complete restoration of the normal anatomy given the restrictions imposed by an artificial material being used to restore the normal bone and joint. The restoration requires ensuring that they muscles are set at the right length and tension. The distance of the centre of rotation of the hip from the pull of the muscles has to be restored to normalcy. Hip biomechanics also has to work like before so that the muscle efficiency is normal and with normal strength. The gait or the walking pattern of these patients has to be restored in a way that they can return to normal efficient walking, without any limp or difficulty.
Most, if not all of these patients after operation are high functioning individuals and can-do activities such as climbing stairs, getting onto the Metro, going on Holidays, taking long walks, doing regular exercises without any issues. For both the patients and the surgeons Total Hip Replacement is a very gratifying operation and life changing.



